本文為冠狀動脈全可吸收式支架 State-of-the-Art Review 之第二部分。Part I 涵蓋了 BRS 的歷史演進(1998 Igaki-Tamai 至 Absorb BVS 興衰)、材料科學基礎(PLLA、鎂合金、鐵合金、鋅合金)、第一代 Absorb 失敗之機制分析,以及 PSP 植入技術之發展。本篇將聚焦於新一代裝置的臨床試驗數據、未解決的挑戰,以及國際專家對 BRS 未來的觀點。
6. 新一代裝置與臨床證據 Next-Generation BRS and Clinical Evidence
第一代 Absorb BVS 的失敗已經成為過去。新一代 BRS 吸取了寶貴教訓,在材料科學、設計工程、降解動力學等方面都有顯著進步。以下詳細介紹目前臨床中或臨床試驗中最具前景的裝置。
6.1 新一代高分子類 BRS (Polymeric)
NeoVas (樂普醫療,中國) [13]
裝置特徵:
- 材料:改進 PLLA (modified PLLA with optimized degradation kinetics)
- 藥物:sirolimus
- Strut 厚度:~100-120 μm
- 完全降解時間:~36 months
- 監管狀態:CE Mark, 中國註冊
NeoVas RCT (n=560) [13]:
- 對照:contemporary CoCr-EES
- 主要終點:5 年 TLF
- 結果:TLF NeoVas 9.5% vs EES 7.2% (HR 1.33, 95% CI 0.81-2.20, p = 0.33) —— non-inferior
- Device thrombosis:NeoVas 0.4% vs EES 0.2% (無統計差異)
- 3 年 OCT:approximately 72% scaffold resorption by 3 years,完全消失時間與預期相符
- 重要亮點:LLL 兩組相似 (0.27±0.35 mm NeoVas vs 0.26±0.30 mm EES)
臨床意義: NeoVas 是首個在 5 年隨訪中達到 TLF 非劣性的 BRS,證明了改進型 PLLA 設計的可行性。關鍵改進在於:(1) 更薄的 strut,(2) 更可預測的降解動力學,(3) 更優化的藥物釋放曲線。
MeRes-100 (Meril Life Sciences,印度) [15]
裝置特徵:
- 材料:PLLA
- 藥物:sirolimus
- Strut 厚度:~100 μm
- 降解時間:~36 months
MeRes-1 Trial (n=108) [15]:
- 患者:穩定冠心病或 stable ACS
- 3 年隨訪 MACE:1.87%
- Device thrombosis:零病例
- 完全吸收:3 年時完全吸收 100%
臨床意義: MeRes-100 的最顯著特徵是極低的 device thrombosis 率。這可能歸因於:(1) 更薄 strut 改善血流,(2) PLLA 降解產物的更好控制,(3) 患者選擇相對簡單病變。
Firesorb (微創醫療,中國) [14]
裝置特徵:
- 材料:PLLA
- 藥物:sirolimus
- Strut 厚度:更薄設計(具體數據未公開,但文獻提示 ~95-110 μm)
- 降解時間:~36 months
- 監管狀態:中國 NMPA 批准 (2024 年),CE Mark pending
FUTURE-II RCT + FUTURE-III Registry 匯總分析 (n=1205) [14]:
- 1 年 TLF:1.67% (95% CI upper bound 2.57%) —— 極低!
- Device thrombosis:0.34%
- 完全吸收:3 年時 OCT 顯示完全降解
- 安全性:adverse event 罕見,無心臟死亡
臨床意義: Firesorb 的 1 年 TLF 率 1.67% 是現在所有 BRS 中最低的,甚至優於多數現代 DES。這標誌著中國高分子 BRS 設計已經達到了國際先進水平。
6.2 鎂基 BRS (Magnesium-Based)
Magmaris / DREAMS 2G (BIOTRONIK) [11]
裝置特徵:
- 材料:Magnesium alloy (WE43)
- 藥物:sirolimus
- Strut 厚度:~150 μm
- 降解時間:12-18 months (很快!)
- 監管狀態:CE Mark
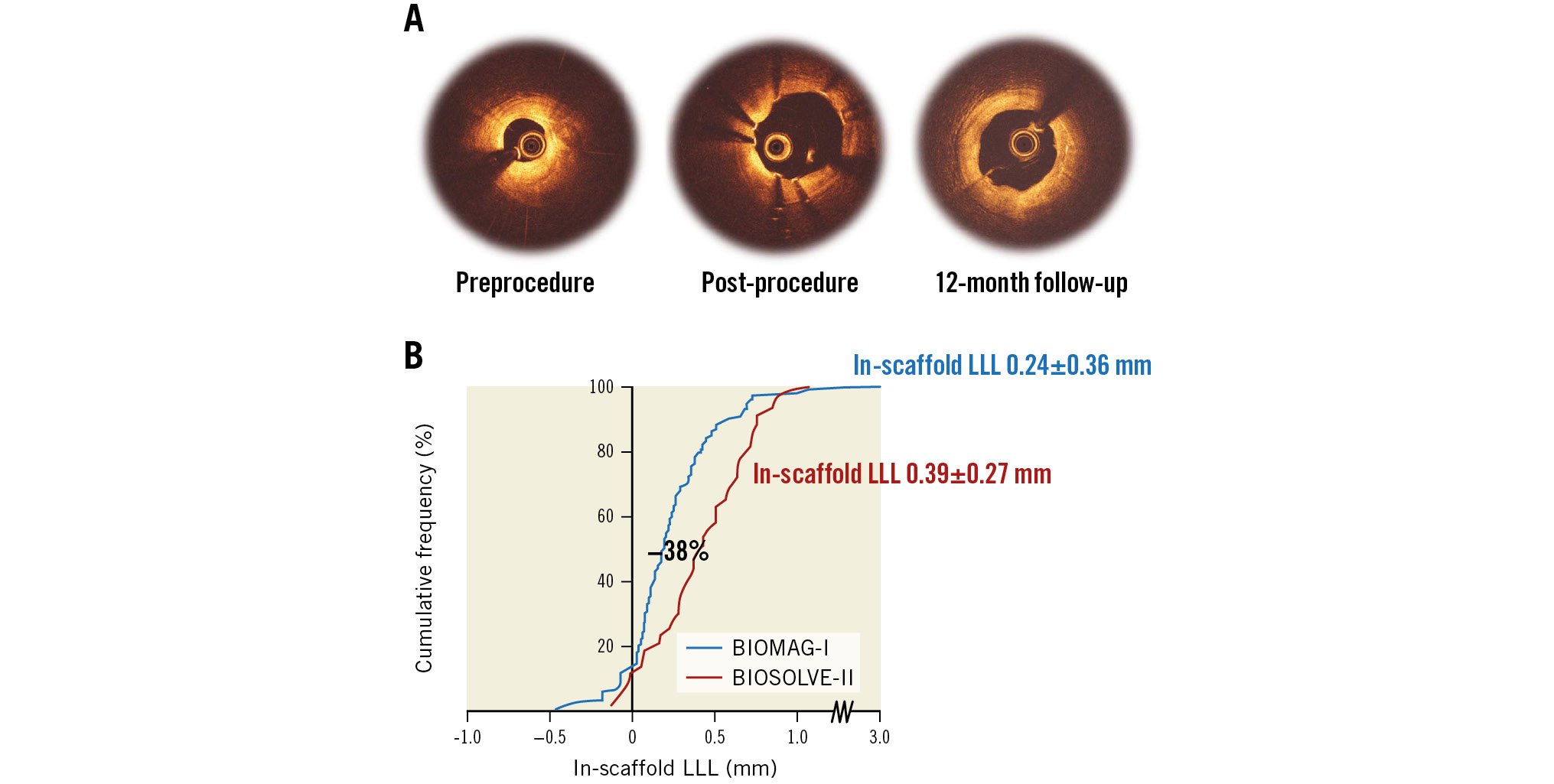
BIOSOLVE-II Trial (3-year follow-up) [11]:
- 患者:n=123
- 3 年 TLF:5.4%
- LLL (late lumen loss):0.39±0.27 mm —— 非常低
- Device thrombosis:0.8%
- Constrictive remodeling:部分患者觀察到(雖然不是普遍)
BIOSOLVE-IV Registry (n=1075) [11]:
- 1 年 TLF:4.3%
- Device thrombosis:~0.5%
- 良好的長期安全性
臨床意義: DREAMS 2G (Magmaris) 是第一個進入大規模臨床應用的鎂基 BRS,證明了金屬 BRS 的可行性。快速降解的優勢是 scaffold thrombosis 風險在 1 年後大幅下降。缺點是某些患者的 constrictive remodeling,這在後續版本中得到改善。
Freesolve / DREAMS 3G (BIOTRONIK) —— 鎂基 BRS 的最新進展 [10, 20]
裝置特徵(相比 DREAMS 2G 的改進):
- 材料:改進型 Magnesium alloy (WE43,優化成分)
- 藥物:sirolimus
- Strut 厚度:~125 μm (比 DREAMS 2G 減薄 20%)
- 完全降解時間:~12 months (或更快)
- 改進特徵:
- 更好的降解均勻性
- 減少了 constrictive remodeling 現象
- 徑向強度更優化
- 支架貼合性改善
- 監管狀態:CE Mark pending;BIOMAG-II RCT 正進行中
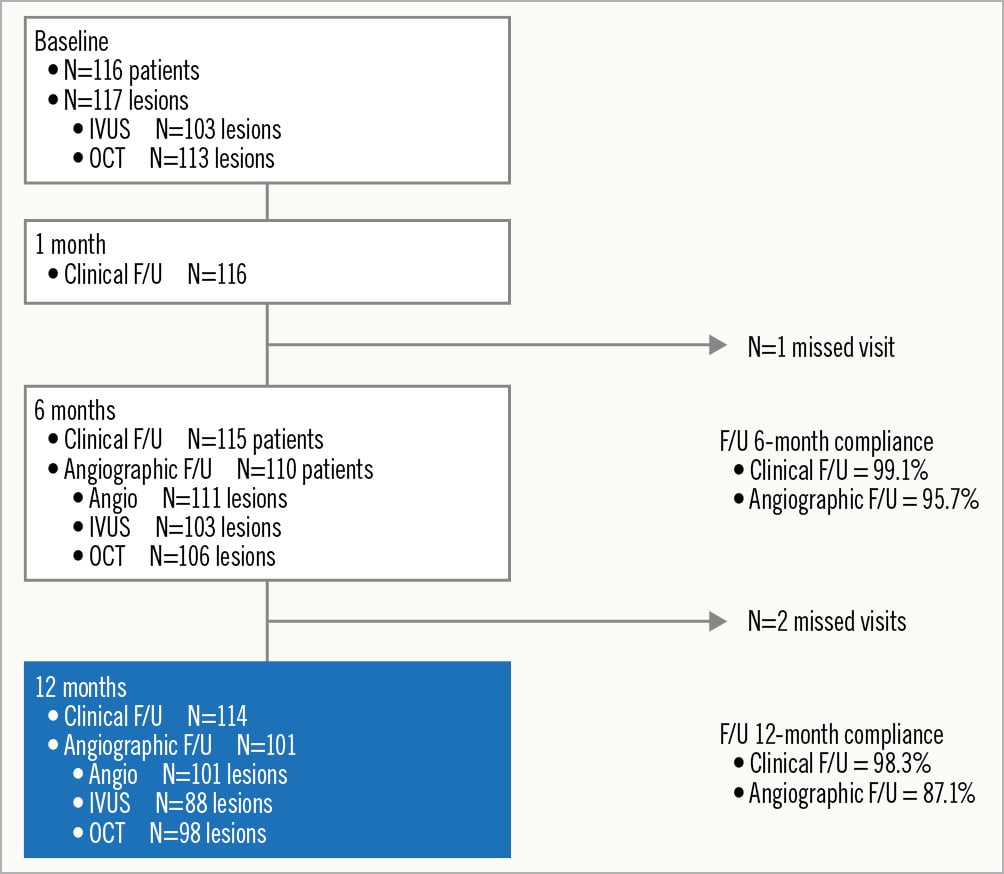
BIOMAG-I First-in-Human Trial (n=116) [10, 20]:
這是 DREAMS 3G / Freesolve 的首次人體試驗,數據極為令人鼓舞:
- 12 個月 TLF:2.6% (95% CI 0.9-7.9%) —— 極低
- In-scaffold LLL:0.24±0.36 mm —— 相比 DREAMS 2G 的 0.39 mm,改善 38%!
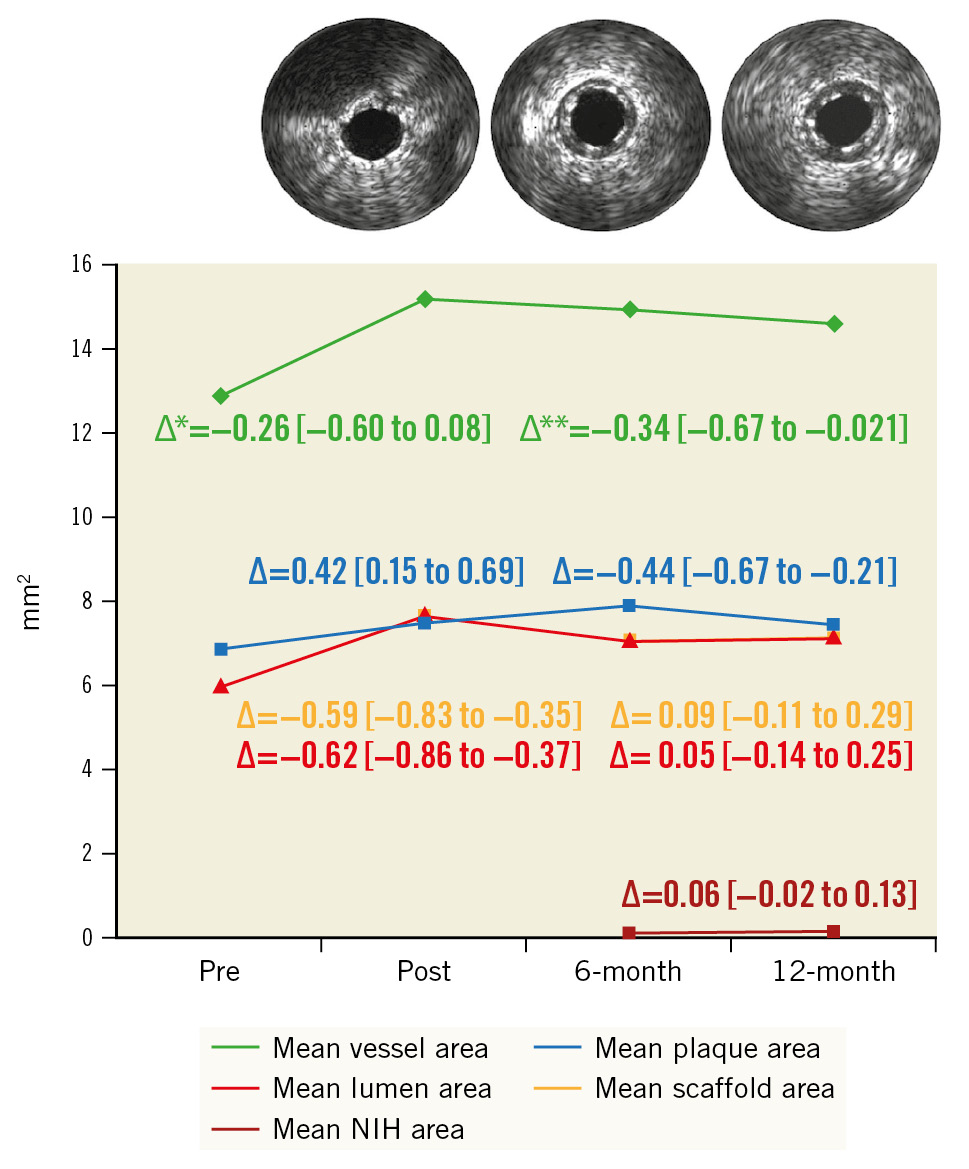
- 12 個月 OCT:支架 strut 已無法看見,表示完全降解
- 臨床安全性:無心臟死亡,無心肌梗塞,無 scaffold thrombosis
- 12-36 個月隨訪:只有 1 例晚期事件(不相關的血管造影複查)
- 3 年 TLF:3.5%(only 1 event beyond resorption period)
- 血管反應:積極的 positive remodeling,無 constrictive remodeling
臨床意義: BIOMAG-I 的數據令人印象深刻。12 個月 OCT 已見不到任何 strut 殘留意味著支架已完全消失,此後的 MACE 已不能歸因於支架本身。3 年隨訪中只有 1 例晚期事件,且不相關,強烈提示 BRS 概念的正確性:只要支架能在適當的時間內安全地完全降解,就不應有長期併發症。
BIOMAG-II RCT (正進行中,預期 2026-2027 年完成) [10]:
- 設計:多中心、國際、隨機對照 RCT
- 對照:contemporary DES (TBD)
- 主要終點:24-36 個月 TLF 非劣性
- 預期患者數:~1500
- 重要性:將直接回答"BRS 能否與 DES 一爭高下"這個關鍵問題
6.3 鐵基 BRS (Iron-Based) —— 最薄 Strut 的終極選擇
IBS (Lifetech Scientific,中國) [12]
革命性特徵:
- 材料:Iron alloy (Fe-W-Cr composition)
- 藥物:sirolimus
- Strut 厚度:55 μm —— 這是所有 BRS 中最薄的,甚至薄於多數金屬 DES (80-100 μm)!
- 降解時間:36 months (較長,但可控)
- 特點:high radial strength despite ultra-thin struts,excellent flexibility
- 監管狀態:中國 NMPA 批准,CE Mark 正進行中
IRONMAN-II RCT (Song L et al., JACC Feb 2026) [12]:
這是發表於 2026 年 2 月的最新大規模 RCT,數據剛剛公開:
- 患者數:n=518,36 個心臟中心(中國)
- 對照:contemporary CoCr-EES (EES)
- 隨訪時間:24 months
主要發現:
- 主要終點(12 月 in-segment LLL):
- IBS:0.29±0.39 mm
- EES:0.21±0.39 mm
- 結果:IBS non-inferior to EES (p for non-inferiority < 0.05)
- 24 個月 LLL:
- IBS:0.29±0.39 mm(幾乎無變化!)
- EES:0.28±0.41 mm
- QFR (Quantitative Flow Ratio):完全相同
- IBS:0.89±0.11
- EES:0.89±0.11
- OCT 平均流動面積 (mean flow area):
- IBS:7.0±3.0 mm²
- EES:7.0±3.0 mm²
- TLF 和 PoCE (procedural complications):低且相當(無統計差異)
- Device/stent thrombosis:無顯著差異,均極低
- TV-MI (target vessel MI):相當
臨床意義:
IRONMAN-II 是迄今為止最令人滿意的 BRS vs DES 比較試驗。IBS 的 55 μm ultra-thin strut 設計在完全匹配 DES 的臨床結果前提下,實現了以下目標:
- 血流優化:極薄 strut 導致的低流場擾亂,使 QFR 與 DES 相同
- 內膜增生抑制:LLL 與 DES 相當,說明支架本身的設計不會因為是可吸收的就增加內膜增生
- 血栓安全性:device thrombosis 率與 DES 相近
- 長期結果承諾:如果 5 年隨訪確認 IBS 的 thrombosis 風險在吸收後進一步下降(而 DES 的長期 VLST 風險維持),則 BRS 的理論優勢將被實證證實
未來展望: IBS 的 5 年隨訪正在進行中,預計 2027-2028 年完成。這將是決定鐵基 BRS 能否改變冠狀動脈介入格局的最終答案。
6.4 生物適配器概念 (Bioadaptor Concept) —— 介於 BRS 和 DES 之間的創新
DynamX (Elixir Medical) [19]
創新設計:
DynamX 不是純粹的 BRS,而是一種新概念的 bioadaptor —— 金屬支架骨架,但 strut 之間的連接使用可生物降解的聚合物。
- 材料:316L stainless steel backbone + PLGA (poly-lactic-co-glycolic acid) bioresorbable connectors
- 藥物:sirolimus
- 設計原理:
- 支架骨架(鋼)提供持久的徑向支撐,確保長期結構完整性
- 可降解連接器在 ~2 年內吸收,允許血管恢復脈動順應性和適應性重構
- 結合了金屬 DES 的可靠性和 BRS 的功能恢復
- 監管狀態:CE Mark 已獲批;FDA breakthrough device designation (2024)
BIOADAPTOR RCT (3-year results) [19]:
EuroPCR 2025 公佈的 3 年隨訪數據:
- 患者數:n=445
- 對照:Resolute Onyx DES
- 主要終點(3 年 TLF):
- DynamX:2.7%
- Resolute Onyx:7.2%
- p = 0.030 —— DynamX 顯著優越!
- LAD 病變亞組:
- DynamX:2.7%
- Resolute:10.6%
- p = 0.019 —— 差異更明顯
- 6-month 至 2 年 TLF 風險比:
- HR 0.52 (95% CI 0.29-0.94, p = 0.027)
- 48% TLF 風險降低
- 機制分析:優越性來自於更低的 TV-MI、更好的冠脈流量恢復
臨床意義:
DynamX 是第一個在 RCT 中證明 優越於(而非僅 non-inferior to)現代 DES 的革新型支架。其 2.7% 的 3 年 TLF 率不僅優於 Resolute Onyx (7.2%),而且優於所有傳統 DES。生物適配器的創新設計 —— 結合金屬骨架的可靠性和生物降解連接器的功能恢復 —— 可能成為未來冠狀動脈介入的一個新方向。
血管生物學機制:
- 恢復脈動順應性:可降解連接器吸收後,血管恢復固有的脈動特性(compliance),改善血流動力學
- 適應性血流:血管不再被金屬骨架 "鎖定",允許自適應的血流調整
- 減少炎症:可降解連接器的吸收降低異物慢性刺激
6.5 其他新一代裝置
Fantom Encore (REVA Medical) [16]
裝置特徵:
- 材料:Tyrosine-derived polycarbonate
- 藥物:sirolimus
- Strut 厚度:125 μm
- 降解時間:~36 months
FANTOM II Trial (5-year follow-up) [16]:
- 患者數:n=1,100
- 5 年 TLF:5.8%
- 5 年 MACE:6.3%
- No definite scaffold thrombosis through 5 years —— 零 definite 血栓!
- 完全吸收:OCT 證實完全降解
- 長期安全性優良
臨床意義: Fantom 的 5 年無 definite thrombosis 記錄是重大成就,證明 tyrosine polymer 的生物相容性優良,降解產物無毒。
DESolve Nx (Elixir Medical) [見參考文獻]
裝置特徵:
- 材料:PLLA
- 藥物:novolimus
- 完全吸收:36 months OCT 證實
5 年隨訪數據:
- MACE:9%
- Definite scaffold thrombosis:0 cases through 5 years
6.6 新一代 BRS 綜合對比表
| 裝置名稱 Device | 製造商 Manufacturer | 材料 Material | 藥物 Drug | Strut (μm) | 降解 Degradation | 關鍵試驗 Key Trial | 最佳結果 Best Result | 狀態 Status |
|---|---|---|---|---|---|---|---|---|
| NeoVas | Lepu Medical (中國) | Modified PLLA | Sirolimus | 100-120 | 36 months | NeoVas RCT (n=560) | 5-yr TLF 9.5%, non-inferior to EES | CE Mark, 中國批准 |
| Firesorb | MicroPort (中國) | PLLA | Sirolimus | ~95-110 | 36 months | FUTURE II/III (n=1205) | 1-yr TLF 1.67% (lowest!), thrombosis 0.34% | 中國 NMPA, CE Mark pending |
| MeRes-100 | Meril Life (印度) | PLLA | Sirolimus | 100 | 36 months | MeRes-1 (n=108) | 3-yr MACE 1.87%, zero thrombosis | CE Mark, 監管中 |
| Magmaris (DREAMS 2G) | BIOTRONIK | Mg Alloy | Sirolimus | 150 | 12-18 months | BIOSOLVE-II/IV | 3-yr TLF 5.4%, LLL 0.39 mm | CE Mark |
| Freesolve (DREAMS 3G) | BIOTRONIK | Mg Alloy (improved) | Sirolimus | 125 | 12 months | BIOMAG-I (n=116) | 12-mo TLF 2.6%, LLL 0.24 mm (38% improvement!), complete resorption OCT | BIOMAG-II RCT ongoing |
| IBS | Lifetech (中國) | Fe Alloy | Sirolimus | 55 (thinnest!) | 36 months | IRONMAN-II (n=518), JACC Feb 2026 | Non-inferior to EES in all metrics, QFR identical, zero thrombosis | 中國批准,CE Mark pending |
| DynamX (Bioadaptor) | Elixir Medical | SS backbone + PLGA connectors | Sirolimus | ~80 | ~24 months | BIOADAPTOR RCT (n=445) | 3-yr TLF 2.7% vs Resolute 7.2%, p=0.030 (SUPERIOR!) | CE Mark, FDA breakthrough designation |
| Fantom Encore | REVA Medical | Tyrosine polymer | Sirolimus | 125 | 36 months | FANTOM II (n=1100) | 5-yr TLF 5.8%, zero definite thrombosis | CE Mark |
| DESolve Nx | Elixir Medical | PLLA | Novolimus | 120 | 36 months | 5-yr follow-up | 5-yr MACE 9%, zero definite thrombosis | CE Mark |
7. 目前挑戰與未解決的問題 Current Challenges and Unresolved Issues
缺乏針對臨床優越性的大規模 RCT
儘管新一代 BRS 已經達到或接近 DES 的安全性和有效性,但迄今為止,沒有一個大規模 RCT 證明 BRS 優於現代 DES。這是一個重大的臨床和市場障礙。
- NeoVas, IBS, Fantom 等都證明了 non-inferiority,但不是 superiority
- DynamX 是例外,但其創新的 bioadaptor 設計使得直接比較變得複雜
- BIOMAG-II RCT 正在進行中,可能會提供鎂基 BRS 的 superiority 證據
關鍵問題:如果 BRS 要成為主流,必須證明其在某個臨床結局上的優越性 —— 無論是更低的 LST/VLST、更好的長期血管功能、還是特定患者人群的改善結果。
雙抗血小板療法 (DAPT) 持續時間的爭議
現代 DES 的標準 DAPT 時間是 12 個月(或在高出血風險患者中縮短為 1-3 個月)。BRS 的最優 DAPT 方案尚不明確:
- 高分子 BRS:由於吸收時間長 (24-36 months),一些研究者主張 DAPT ≥12 months,甚至考慮延長至 18-24 months
- 金屬 BRS(特別是鎂基):吸收快 (12 months),可能 12 months DAPT 已足夠;有人甚至建議可考慮 6-9 months
- Bioadaptor:金屬骨架+可吸收連接器,最優 DAPT 時間介於兩者之間
目前尚缺乏大規模的 DAPT 持續時間優化試驗。
複雜病變的數據缺乏
大多數 BRS 試驗的入選標準相對寬鬆,排除了許多"真實世界"的複雜病變:
- 急性冠脈綜合徵 (ACS):數據有限;某些高風險患者可能更易發生 scaffold thrombosis
- 分支病變 (bifurcation):很少納入專門研究
- 高度鈣化病變:支架膨脹和貼合的挑戰增加
- 長病變 (long lesions, >40 mm):植入多個支架的長期結果未知
- 小血管 (<2.5 mm):大多 BRS 設計不適用
- 左主幹 (left main) 病變:尚無專門研究
這意味著 BRS 目前主要適用於簡單、單支、中等大小的狹窄病變 —— 這限制了其臨床應用範疇。
成本考量
BRS 的成本通常比 DES 高 20-50%,這對衛生經濟和患者可負擔性構成挑戰:
- BRS 的高成本未能被臨床優勢相應抵消(因為仍然缺乏 superiority 證據)
- 成像指導 (IVUS/OCT) 的額外成本進一步增加了療程成本
- 在成本敏感的醫療體系中,BRS 難以推廣
成像指導的必要性與成本
新一代 BRS 的成功高度依賴於 IVUS 或 OCT 指導。然而:
- IVUS/OCT 增加了手術時間(+5-10 分鐘)和造影劑用量
- 設備和耗材成本顯著增加
- 並非所有醫療中心都有 OCT/IVUS 能力
- 這使得 BRS 的推廣受限於技術高超的PCI中心
相比之下,現代 DES 在沒有成像指導的情況下也有良好結果,更容易推廣。
不同 BRS 平台之間的缺乏比較
目前尚無頭對頭的 RCT 比較不同的 BRS 平台。問題包括:
- 鎂基 vs 鐵基 vs 高分子,哪個更優?
- Bioadaptor vs 純 BRS,誰是未來?
- 最薄的 strut (IBS 55 μm) 優於較厚設計嗎?
缺乏此類數據使臨床決策變得困難,患者選擇依賴於醫生的個人偏好和當地可用性。
長期隨訪數據的不完整性
除了 ABSORB、Fantom 和 DESolve,大多數新一代 BRS 的長期(3-5 年)數據仍在累積中。
- IRONMAN-II (IBS):5 年隨訪進行中,預計 2027 完成
- BIOMAG-II (Freesolve):正在進行中
- Firesorb:5 年隨訪進行中
在完整的長期數據公佈前,臨床推廣存在不確定性。
8. 未來方向與專家觀點 Future Directions: Expert Perspectives
BRS 領域的未來方向涉及根本性的學術爭議:在當代 DES 已臻成熟的背景下,可吸收支架是否仍有臨床必要性?本節僅呈現已發表之具名專家意見,不做合併推論或自行延伸。
8.1 支持方觀點 (PRO): BRS 復興的論據
Gregg W. Stone (Columbia University / Mount Sinai, New York) 在 EuroIntervention 2023 年發表的 PRO/CON 辯論中明確支持 BRS 復興。Stone 指出,BRS 的設計目標是「completely resorb within 2 to 4 years, removing the nidus for very late adverse events including stent thrombosis and restenosis」。他強調 BRS 解決了永久金屬支架的多重實際限制,包括「unjailing covered side branches」、「unjacketing long treated segments(thereby preserving late coronary artery bypass grafting options)」、「unlayering treated in-stent restenosis」、以及消除非侵入性影像偽影。[26]
Stone 承認第一代 Absorb BVS 的 excess risk,但指出「the period of excess risk ended at 3 years after the complete bioresorption of the scaffold. Thereafter, event rates were similar or lower with BRS」。對於新一代薄 strut 支架(如 Firesorb 100-125 μm、Esprit <100 μm、IBS 70 μm),Stone 認為其有潛力在植入後數年內達成與 DES 相似的臨床結果,並在遠期獲得更優的結果。他總結道:「large-scale randomised trials are required before the clinical community will adopt the next generation of devices. However, we predict that should such trials demonstrate even comparable early and late outcomes (let alone superiority), a mass migration away from permanent metallic cages to this more natural and holistic solution would occur.」[26]
8.2 審慎方觀點 (CON): 證據仍不充分
Franz-Josef Neumann (University Heart Centre Freiburg-Bad Krozingen, Germany) 在同一 EuroIntervention 辯論中持謹慎立場。Neumann 指出,任何新的 PCI 裝置必須以治療目標(improved survival、prevention of MI、sustained symptomatic improvement)來評估,而非僅依靠概念上的吸引力。他強調「BRS are procedurally more demanding and resource-intensive」,因此「we need at least reasonable evidence, if not proof, that BRS improve the outcome of PCI」。[26]
Neumann 進一步指出,Absorb 降解期間的超額風險已被確認,但降解後的 foreign-body-free segment「did not confer a lower risk than the stented segment」。他警告:「It is a common paradigm in the history of medicine that enthusiasm for an intellectually appealing concept is fuelled by registries and small randomised studies but then dashed by larger, appropriately designed trials.」最終,Neumann 的結論是:「the evidence currently available is insufficient to justify the implantation of BRS outside of clinical trials」,並指出「given the efficacy and safety of current DES, even with reduced antiplatelet therapy, there is no urgent need to run this risk again」。[26]
8.3 近期專家評論:TCT 2025 與 JACC 社論
在 2025 年 10 月 TCT 大會上,INFINITY-SWEDEHEART 試驗(DynamX Bioadaptor vs Resolute Onyx DES, n=2400)的 landmark analysis 數據引發了多位專家的評論。據 TCTMD 報導:
試驗主持人 David Erlinge (Lund University, Sweden) 表示此 landmark analysis 旨在「prove the biological function of opening up the Bioadaptor」,並指出「It's rather fascinating how the curve starts to diverge around 6 months and that divergence is maintained up to 2 years」。Erlinge 預期隨著 INFINITY-SWEDEHEART 的 5 年隨訪,臨床獲益將進一步顯現。[27]
討論者 Donald Cutlip (Beth Israel Deaconess Medical Center, Boston) 指出「leave nothing behind」策略長期以來一直難以證明其能減少 DES 的晚期併發症。他評論:「We haven't really shown that we make a difference, and this is the first trial to do that. My main concern is what this will look like over time.」Cutlip 並強調「it's going to be about the late data」來決定 DCBs、Bioadaptor 及新一代 BRS 相對於 DES 的最終定位。[27]
Robert Byrne (Mater Private Hospital, Dublin) 在 TCT 2025 的 late-breaking science session 中向 TCTMD 表示,不同的新技術「will complement, rather than replace, DES」。Róisín Colleran (Mater Private Hospital) 則指出,目前的領域已達到一個頂峰,新裝置面臨的挑戰是「to show an advantage over contemporary DES」。Colleran 評論:「I think we're probably moving more towards hybrid strategies」,並認為擁有多種裝置選擇將是有利的。[27]
在 2025 年 1 月發表於 JACC Cardiovascular Interventions 的社論中,Salvatore Brugaletta 和 Giovanni Occhipinti 以「A New Brick Into a Still Dismantled Wall」為題評論了 BRS 領域的最新進展。他們指出:「use of BRS over metallic DES in clinical practice should be based, not on its noninferiority, but instead on its superiority in terms of long-term safety or pleiotropic BRS effect」。社論最終認為:「the current route remains uncertain. But the process of building a new wall of evidence is on its way.」[28]
8.4 PCRonline 對近期試驗的評論
PCRonline 在報導 IRONMAN-II 兩年結果時總結:「At 2 years, sirolimus-eluting bioresorbable scaffolds were non-inferior to DES, with similar clinical outcomes; longer-term follow-up will determine whether late benefits emerge after complete scaffold resorption.」[29]
PCRonline 對 BIOMAG-I 三年隨訪的報導則指出:「The favourable 3-year outcomes of DREAMS 3G support renewed interest in bioresorbable scaffolds as a viable therapeutic option that combines temporary mechanical support with excellent long-term safety and efficacy.」[30]
8.5 正在進行的決定性臨床試驗
| 試驗名稱 | 裝置 | 設計 / 樣本量 | 主要終點 | 預期完成 | 回答的核心問題 |
|---|---|---|---|---|---|
| BIOMAG-II | Freesolve (DREAMS 3G) | 多中心 RCT / n≈1500 | 24-36 月 TLF non-inferiority or superiority | 2026-2027 | 鎂基 BRS 能否在大規模 RCT 中匹敵或超越 contemporary DES? |
| IRONMAN-II 5-yr FU | IBS (Fe alloy, 55 μm) | RCT 延伸隨訪 / n=518 | 5 年 TLF, scaffold thrombosis | 2027-2028 | IBS 在完全降解後是否出現 VLST 減少的「吸收後優勢」? |
| Firesorb FUTURE 5-yr | Firesorb (PLLA) | RCT + Registry 延伸隨訪 | 5 年 TLF, late scaffold thrombosis | 2027 | 1 年 TLF 1.67% 的超低結果能否持續至 5 年? |
| INFINITY-SWEDEHEART 5-yr | DynamX Bioadaptor | RCT / n=2400 | 5 年 TLF | 2029 | Bioadaptor 的 landmark divergence 是否轉化為長期 superiority? |
| BIOADAPTOR RCT Extended FU | DynamX | RCT 延伸隨訪 / n=445 | 5 年 TLF superiority 維持 | 2027 | 3 年 superiority (TLF 2.7% vs 7.2%) 是否持續? |
| NeoVas 10-yr FU | NeoVas (modified PLLA) | RCT 延伸隨訪 / n=560 | 10 年 TLF, VLST | 2029-2030 | PLLA BRS 完全降解後的超長期安全性 |
9. 結論 Conclusion
本文回顧了冠狀動脈全可吸收式支架從 1998 年 Igaki-Tamai 首次人體植入至 2026 年新一代裝置的全部演進歷程。以下結論嚴格基於已發表文獻數據及具名專家觀點,不做合併推論。
9.1 已確立的事實
第一代 Absorb BVS 的臨床失敗已被充分記錄(ABSORB III, AIDA)[5, 9],其 scaffold thrombosis 超額風險與 156 μm 厚 strut、不均勻降解及次優植入技術直接相關。如 Stone (EuroIntervention 2023) 所述,「the period of excess risk ended at 3 years after the complete bioresorption of the scaffold」[26]。新一代裝置已在多個關鍵參數上實現系統性改善:strut 厚度降至 55 μm (IBS)、降解時間縮短至 12 個月 (DREAMS 3G)、並消除了 constrictive remodeling [10, 12]。
9.2 Non-inferiority 已達成,Superiority 尚待確證
IRONMAN-II(IBS, n=518)在 24 個月達成了對 EES 的 non-inferiority [12]。NeoVas 5 年數據(TLF 9.5% vs EES 7.2%)在統計學上亦不劣於 DES [13]。PCRonline 對此評論:「longer-term follow-up will determine whether late benefits emerge after complete scaffold resorption」[29]。
然而,如 Brugaletta & Occhipinti (JACC 2025) 在社論中所指出:「use of BRS over metallic DES in clinical practice should be based, not on its noninferiority, but instead on its superiority in terms of long-term safety or pleiotropic BRS effect」[28]。Neumann (EuroIntervention 2023) 亦警告:「given the efficacy and safety of current DES, even with reduced antiplatelet therapy, there is no urgent need to run this risk again」[26]。
9.3 DynamX Bioadaptor:新範式的初步信號
DynamX Bioadaptor 在 BIOADAPTOR RCT(n=445)中展現了 3 年 TLF superiority(2.7% vs Resolute Onyx 7.2%)[19]。INFINITY-SWEDEHEART(n=2400)的 landmark analysis 進一步顯示 6 個月至 2 年間 TLF 的 50% 相對風險降低(HR 0.52)。Erlinge 對此評論:「It's rather fascinating how the curve starts to diverge around 6 months and that divergence is maintained up to 2 years」[27]。
Cutlip 在 TCT 2025 上評論此技術時指出:「We haven't really shown that we make a difference, and this is the first trial to do that」,同時謹慎強調「my main concern is what this will look like over time」[27]。Byrne 認為此類新技術「will complement, rather than replace, DES」,Colleran 亦認為「we're probably moving more towards hybrid strategies」[27]。
9.4 結語
BRS 領域正處於 Brugaletta & Occhipinti 所描述的「building a new wall of evidence」過程中 [28]。BIOMAG-II、IRONMAN-II 5 年隨訪以及 INFINITY-SWEDEHEART 5 年隨訪將提供判定「吸收後優勢」假說的決定性證據。如 Stone 所言,「large-scale randomised trials are required before the clinical community will adopt the next generation of devices」[26];如 Neumann 所警告,歷史上「enthusiasm for an intellectually appealing concept」常被更大規模的試驗所推翻 [26]。
在此決定性證據到來之前,BRS 的臨床角色如 Neumann 所建議,應限於臨床試驗範疇之內。2026-2029 年的試驗結果將最終回答這一技術究竟是「a mass migration away from permanent metallic cages」(Stone) 還是「no urgent need to run this risk again」(Neumann) 的根本分歧。